Scroll down to see the most commonly asked questions are their respective answers. You can find more information on KLM's prescription and over-the-counter products, as well as KLM's prescription special additions and accommodations by clicking the link below...
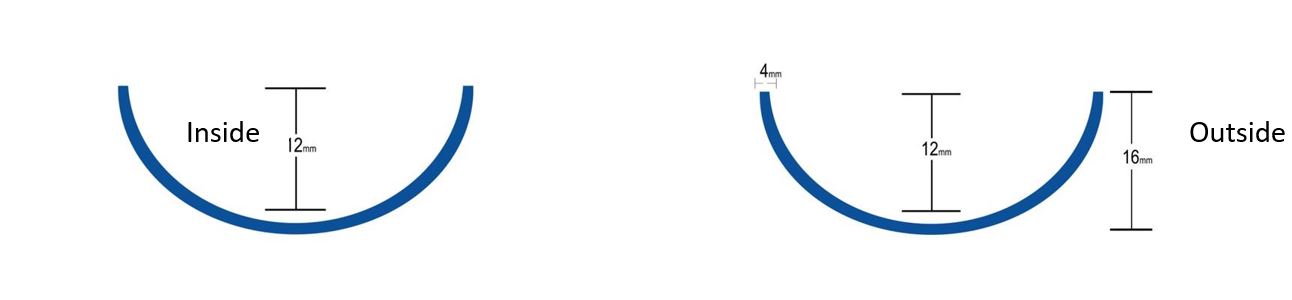
What is the Heel Cup? The vast majority of variables are in the heel area. It is best to begin with the heel cup height.
Most labs choose their standard heel cup height based on gender and shoe type. Typically, men’s orthotics have a 12 mm heel cup and women’s have a 10 mm heel cup. This is because women’s shoes are usually less accommodating for orthotics. The higher heel cup has a tendency to lift the heel higher in the shoe and also makes the orthotic wider, making it difficult to fit comfortably in fashion or tight fitting shoes.
Most sport related orthotics have a 14 mm heel cup. Luckily, most sport and work shoes now have removable insoles, which provides more options that will increase control and not create shoe fit problems.
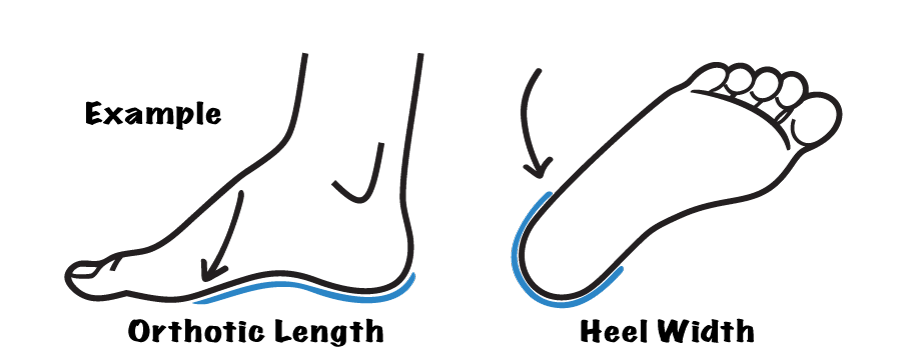
KLM’s standard is to measure the heel cup from the table to the posterior edge.
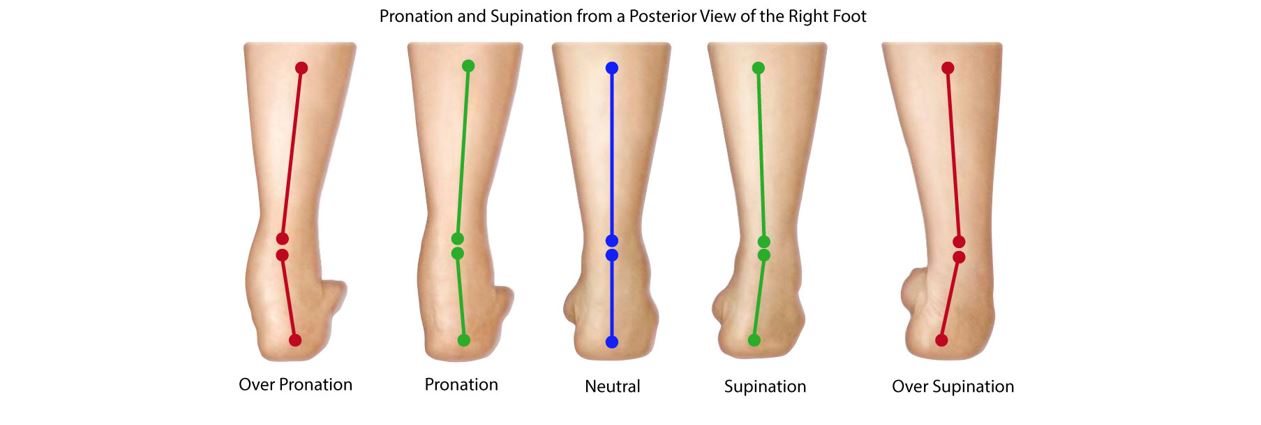
What is pronation and supination? Pronation involves a combination of three motions: Eversion, Abduction and Dorsiflexion.
Supination involves a combination of three motions: Inversion, Plantarflexion and Adduction.
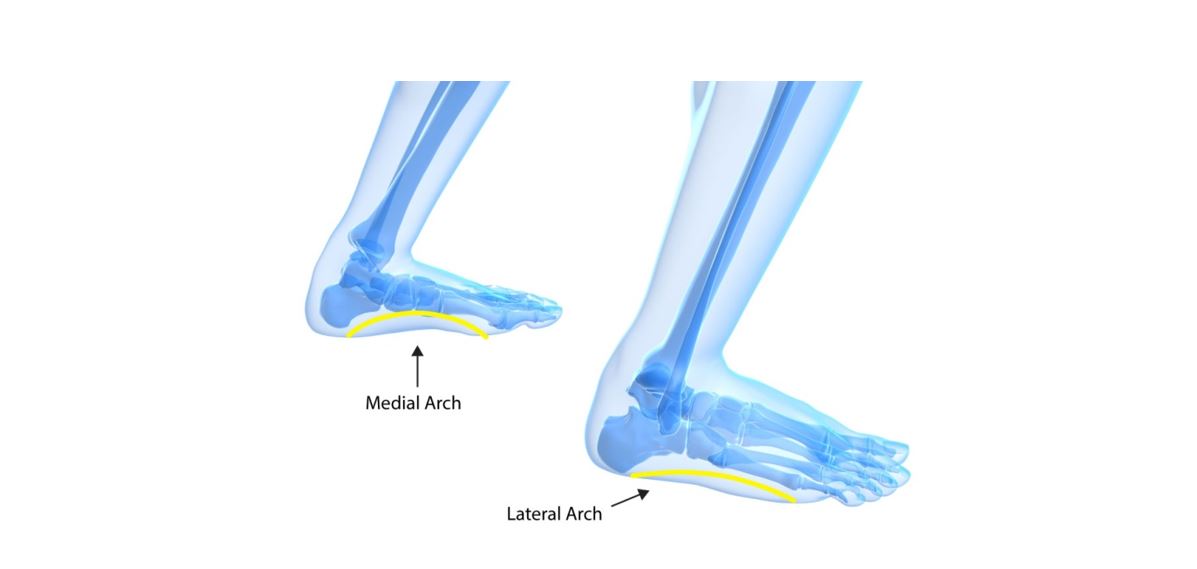
What are the medial and lateral arches? The medial arch is located along the inside edge of the foot, or the edge along the first metatarsal.
The lateral arch is located along the outside edge of the foot, or the edge along the fifth metatarsal.
What is the Transverse Arch? The transverse arch is created behind the metatarsal heads running medial to lateral.
What is a Medial Flange? Medial Flanges are added to increase orthotic stiffness and pronation control. This is achieved by rounding up the medial aspect of the arch correction and shaping the device so that it wraps medially up around the first ray and talar/navicular (TN) area. Medial flanges are usually accompanied with a higher medial heel cup.
Medial flanges, however, can create shoe fit problems in adult shoes. And most adults cannot tolerate the additional stiffness and control. Medial flanges are used most often with children and are an integral part of a standard UCBL type device.
Also look for a TN bulge on your pes planus patients during mid-stance. You will need to accommodate it in the flange correction, creating a pocket to accommodate the TN bulge. It also helps to add a little padding in the pocket.
What is a Lateral Flange? Lateral Flanges help prevent the patient’s foot from sliding laterally off of the orthotic and also resist unwanted supination during the stance phase of gait. Lateral flanges are usually accompanied with a higher lateral heel cup and especially useful for patients with increased transverse compensating mid-tarsal joints, and for increased medial-lateral control at mid-stance.
Lateral flanges also increase the bulk of the device and make it difficult to fit properly in most adult shoes. Lateral Flanges, like Medial Flanges, are typically used more for children and are an integral part of a standard UCBL type device.
What is a Lateral Skive? A lateral skive causes a pronatory moment from heel contact through the early stance phase of gait and thus creates resistance to supination, much like a flat or everted rear foot post. Combining an increased lateral heel cup height with a lateral flare on the rear foot post, and a lateral skive are excellent options for patients who have a tendency for lateral ankle sprains.
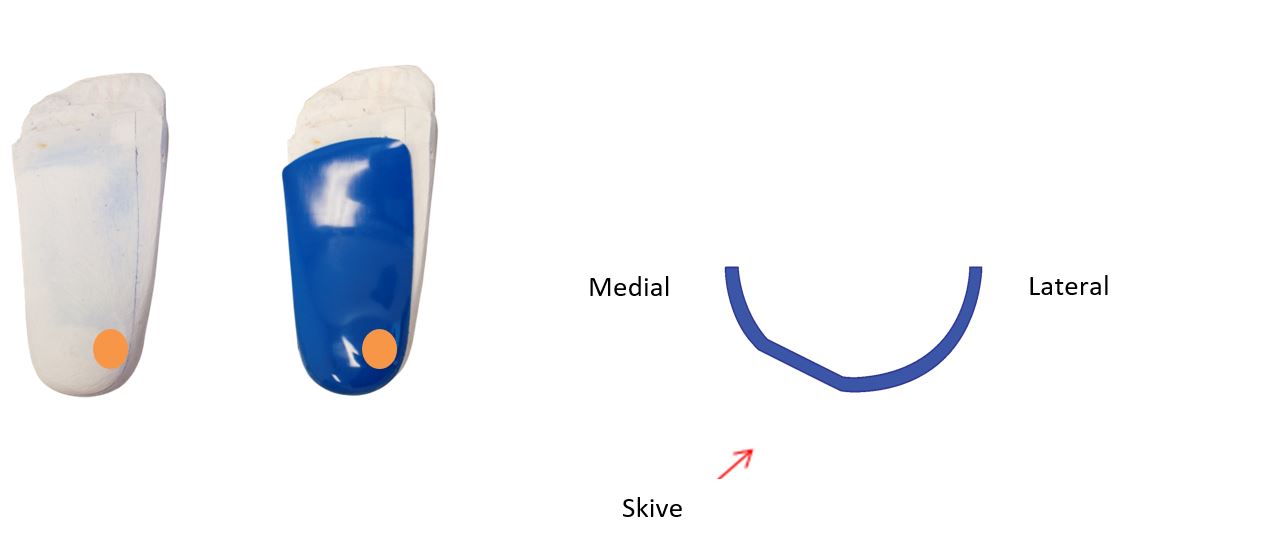
What is a Medial Skive? Medial Skives involve flattening the heel area under the medial aspect of the positive cast, or mold, generating a corresponding flat shape on the orthotic under the medial posterior aspect of the calcaneus.
Medial skives create a supinatory moment from heel contact through the early stance phase of gait and thus create additional resistance to pronation, as with an inverted rear foot post. Studies have also shown that skives can be more effective than rear foot posts. Skives are also a great option when the patient’s shoes cannot accommodate a rear foot post. Combining an increased medial heel cup height with a medial flare on the rear foot post, and a medial skive are excellent options for heavy pronators.
What is a Forefoot Accommodation? A Forefoot accommodation will off load sore tender areas, IPKs, lesions, callouses, etc. A padded extension is added to the distal edge of the device that extends to either the sulcus groove or the end of the toes. Then another pad is added that has cut outs for areas that need to be offloaded. You choose the material, the durometer, and the thickness of both the extension and the cut out pad. Forefoot accommodations are often combined with a met pad to lift the metatarsal proximal to the area to be offloaded.
What is a Styloid Process Accommodation? For patients with a large or tender styloid process on the base of the 5th metatarsal, order a Styloid Process accommodation. The lab will add additional expansion laterally around the base of the 5th met and also under it. The resulting orthotic will have a pocket for the Styloid Process to fit into comfortably. You also can add soft foam in the pocket to provide additional comfort. Styloid process accommodations also are useful with patients who tend to subluxate the lateral column at the cuboid 5th metatarsal joint during heel off and into propulsion.
What is a Morton's Extension? A Morton’s Extension is indicated for a structural elevatus of the 1rst ray, which causes the 2nd metatarsal head to bear weight excessively because the 1rst ray cannot plantarflex in late mid-stance and propulsion. Its purpose is to preload the first metatarsal head and hallux and balance the load on the 2nd ray. Very useful for structural hallux limitus and rigidus, or whenever motion at the 1rst metatarsal phalangeal joint is not desired. The Morton’s Extension supports the 1rst metatarsal head and hallux in relation to the 2nd through 5th metatarsal heads and engages the windlass mechanism in late stance and propulsion.
What is a "Dancer's Pad" or "Kinetic Wedge"? A Dancer’s Pad or Kinetic Wedge is usually ordered to treat Functional Hallux Limitus.
Similar to a forefoot accommodation of the 1rst metatarsal head, the pad lifts 2 through 5 metatarsal heads, allowing the 1rst metatarsal to drop and function below the others, thus enabling 1rst metatarsal phalangeal joint dorsiflexion. Usually combined with a medial tip grind and a flat forefoot post to further allow the first ray and hallux to function below 2 through 5.
What is a Varus or Valgus Wedge? Varus or Valgus Wedges are added to carry the correction from the orthotic forward to the sulcus groove or the end of the toes. For example, if a 5 degree forefoot varus correction is added to the positive cast to invert the forefoot on the rear foot, this correction ends at the distal edge of the orthosis. Once the heel comes off the ground during gait, the correction is lost. So if rear foot control does not result in the medial column plantar-flexing during propulsion, undesired pronation will occur from heel off through propulsion.
Adding a 5 degree Varus Sulcus Wedge extends this correction beyond the distal edge of the orthotic and maintains the correction through heel off and propulsion. It is paper thin under the 5th metatarsal and up to 1/4 inch (6mm) under the 1rst metatarsal.
Similarly a Valgus Wedge is used to carry a valgus correction to the sulcus groove or the end of the toes. It is paper thin under the 1rst metatarsal and up to 1/4 inch (6mm) under the 5th metatarsal.
Valgus wedges are very effective for increasing 1rst ray stability and engaging the windlass mechanism.
Varus and Valgus wedges fill the toe box of the shoe and are only recommended for patient’s whose shoes have removable insoles. In addition, the amount of wedging available is limited by how much room is available in the toe box of the shoe.
Orthotic Wearing Instructions? Wear your orthotics for up to one hour the first day, two hours the second day and gradually more often if comfortable, or less if necessary. If your orthotics cause pain before you have worn them for the scheduled period, remove them. On the next day, Do not attempt to increase the wearing time. Then resume your schedule the following day, increasing the wearing period 1 hour per day. Click here to read more about orthotic wearing and fitting.
What is a Heel Lift? You can also add Heel Lifts to rear-foot posts. Lifts are often added to the prescription for a limb length discrepancy. They also can be used to address a patient’s equinus condition, especially osseousis equinus or forefoot equinus. Shoes with removable insoles allow you to elevate the heel in the shoe up to about 1/4 inch (6mm) and most labs recommend never going higher that. Extra depth shoes allow for even higher heel lifts, or lifts that raise the heel, arch, and forefoot areas of the foot simultaneously–which is the best way to accommodate a limb length discrepancy.
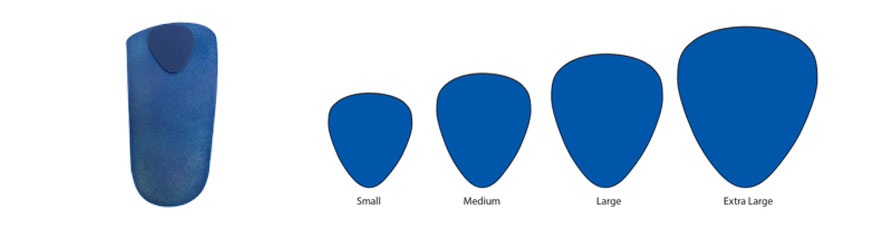
What is a Metatarsal Bar? Metatarsal Bars (Met Bars) are pads that lift and cushion all five metatarsal heads simultaneously. Met bars are excellent for adding additional shock absorption at the metatarsal heads or for engaging the foot’s windlass mechanism. You choose the material, the durometer, and the thickness of the Met Bar.
What is a Metatarsal Pad?A tear drop build up on the dorsal distal portion of the foot orthotic that is highest in the middle and tapers away the edges. The met pad elevates specific metatarsal heads to reduce pressure on the met head. Standard met pad height is 1/8” and placed behind the third met head. They come in different sizes and thicknesses.
What is a Fascial Band Accommodation needed? Fascial Band Accommodations are added when patients have a flexible anterior cavus causing the Hallucis Longus Tendon (HL) to “bowstring” at heel off, irritating the medial arch of the foot. You can test for this by dorsiflexing the first toe and watching the HL under the first/second metatarsals.
What is a heel spur accommodation? Both horseshoe cut outs and donut cut outs are very effective for offloading heel spurs or pain from plantar fasciitis. Most labs recommend no more than 1/8th inch (3mm) thick heel pads because they lift the heel higher in the shoe causing shoe fit problems. Also available is the intrinsic heel spur accommodation, pictured right, for which a delve is made in the shell and filled with a soft material.
What is a Toe Crest? A Toe Crest is ordered when you want to fill the sulcus groove. Toe crests can be ordered from soft materials such as poron and low durometer EVA foams, or from firm materials such as cork or high durometer EVA foams. Toe Crests are very effective for stabilizing and supporting rigid or semi-rigid hammertoes. They often are used in combination with other special features to help stabilize the foot from heel contact through mid-stance and into propulsion.
What is a Rear Foot Post? Rear foot posts are usually added to resist and control heel contact pronation from heel contact through the early stance phase of gait. Posts are usually made from hard rubber or EVA foams. Many standard orthotics designs come with rear foot posts, such as most sports orthotics. Rear foot posts are also an excellent option for patients with a low subtalar joint axis, or whenever there is significant subtalar joint motion in the frontal plane.
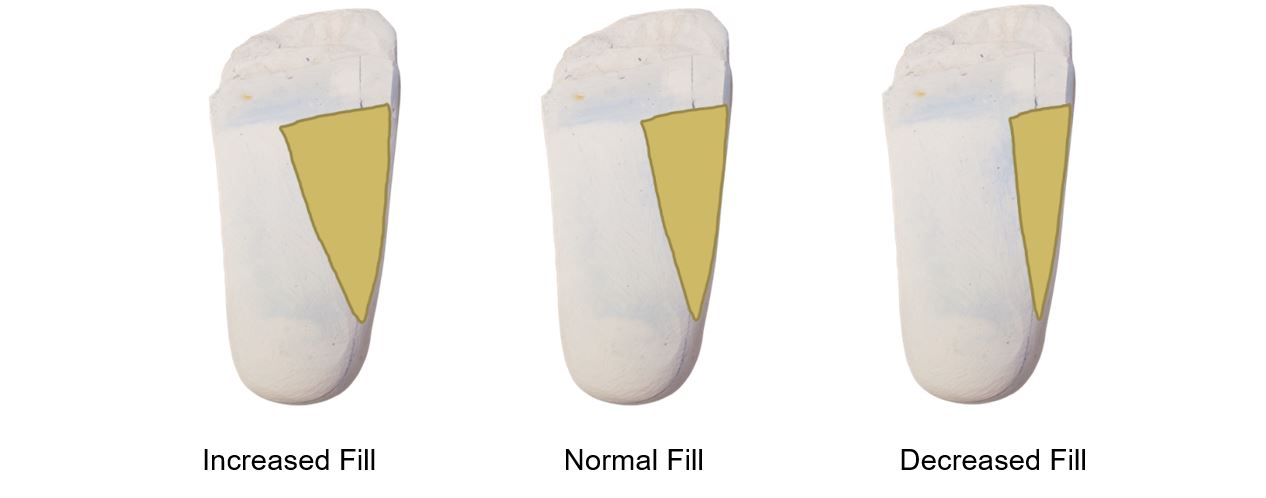
What is the role of Medial Arch Fill? The role of the Medial Arch Fill is to flare the medial edge of the orthotic away from the foot’s natural contour to allow for some flattening of medial arch. You can increase or decrease the medial arch fill on the positive mold based upon patient need.
Increasing the arch fill will lower the medial arch height of the orthotic and allow the foot to pronate more on the device. This can be especially helpful for older patients or obese patients who cannot tolerate full correction.
Decreasing the arch fill will raise the medial arch height on the orthotic, allowing for a closer fit to the foot’s medial arch and provide more control of pronation and the foot in general—most often used for kids, young adults, and athletes.
Thus, the height of the arch directly affects the stiffness, or rigidity, of the orthotic shell. See the arches below. Both have the same width and thickness. The higher arch will be stiffer or more rigid because of the increased curvature. This rule applies to all spring like arches.
Clinical pearl: by ordering less Medial Arch Fill, you can get the same stiffness out of an orthotic from a thinner plastic plate, or a more flexible composite weave. By ordering more Medial Arch Fill, you get a more flexible (less stiff) orthotic.
Does KLM offer discounts or other ways of reducing the cost of custom prescription orthotics? Due to the hands on labor required to construct custom orthotics, quantity discounts are not available. However, KLM has devised multiple ways of reducing the labor and cost of orthoses. Historically, custom neutral position orthotics were made by converting the negative casts of a patient’s feet into positive plaster molds. The orthotics were then pressed to the corrected molds to create a handmade custom device. This technique is known as “Hand Corrected” and is the most labor intensive way to make custom foot orthotics, also making it the most expensive. The innovators at KLM Labs developed another technique called “System_Rx.” This computerized cast correction system uses the critical data from the patient’s negative casts. Per the practitioner’s prescription, corrections are added and the computer generates a positive mold to which the custom orthotic is pressed. Removing some of the labor required for the Hand Corrected technique, System_Rx allows for reduced costs without compromising accuracy. KLM Labs has expanded on the “System_Rx” correction technique by creating the “Value System_Rx” orthotic shells. After monitoring System_Rx and discovering that 99 shapes repeated themselves more than 70% of the time, KLM built these 99 shapes as plastic injection molds. Now these common shapes can be injection molded as polypropylene shells available in 3 rigidities. While these shells are not recommended for patients with severe foot deformities, they are very effective for patients with normal foot types. The less labor required to make the orthotic shell, the greater savings for the practitioner.
For the benefit of practitioners and patients alike, all of KLM’s Rx Foot Orthotics can be made by shoe size. Yes, that means all of the Sport, Fashion, Geriatric, Pediatric and Diabetic custom orthotics. If for whatever reason, casts of the patient’s feet are not available, or the patient cannot afford custom orthotics, simply check the box labeled “California Preform” in the upper right hand corner of KLM’s Rx form and include the patient’s shoe size. Also, enjoy the California Preform discount! Questions? Don’t hesitate to contact our world class customer service team by email at [email protected] or by phone at 800-556-3668.
What is the role of Lateral Arch Fill?The purpose of the Lateral Correction is to account for fat pad expansion along the heel and lateral border during weight bearing. Typically added to non weight bearing casts or digital scans. So it is important to identify patients with excess fat or who lack tissue tone in the heel area, when considering how much lateral correction to request. Excess fat add more. Lack of fat tissue, add less.
What is KLM's return policy? All KLM custom prescription orthotics have a warranty against defects in materials and workmanship beginning on their ship date from KLM Labs. KLM warranties the shell material for six months and the covers and soft materials for 90 days. KLM cannot issue credits due to patient non-compliance, non-tolerance, non-acceptance, or reimbursement failures. Adjustments to orthotics are covered within the first six months, for example, raising or lowering arches and shortening orthotics. Changes to the original prescription are not covered. Examples of adjustments not covered are but are not limited to adding an accommodation which was not originally requested or changing the orthotic type. Over-The-Counter Product returns must be authorized in advance and free from wear (in new condition). Customer pays return shipping along with a restocking fee. Modified products are not eligible for return. Please submit return requests in writing to [email protected], or call customer service at 800-556-3668 during normal business hours. If a return is authorized, options will be provided. If a return is ineligible, the reason will be specified.
Does KLM have a product guarantee? Yes! All KLM products come standard with a 6 month guarantee. The guarantee protects against defects in materials and workmanship. Plastic and metal parts are guaranteed for 6 months while soft materials like covers and posts are guaranteed for 90 days from the ship date from KLM Labs. Unfortunately, KLM cannot issue credit due to patient non-compliance, non-tolerance, non-acceptance, or reimbursement failures. Adjustments to custom orthotics orthotics are covered within the first 6 months; for example, adjusting arch heights or shortening orthotics. Changes to the original prescription are not covered. For example, adding an accommodation that was not originally requested or changing the orthotic type is not covered. Click here to read more about KLM's Provider Policies.